
Following this just past long holiday weekend, the outcome of settling back into a predictable weekend rhythm of data collection and reporting remains unsettled. There are hints that the rate of new cases is slowing, but last week (Sunday, Jan. 10th through Saturday, Jan. 16th) had the second highest weekly count, second only to the just prior week. Our 7-Day average of new cases has been falling from its record high for the last 5 days, but the 14-Day average remains at its highest levels. At the current rate of new cases, we will end January with over 100,000 cases for that single month– a new record high. The Aggregate Total Number of cases continues to climb exponentially. If nothing else changes, we could reach a total of 500,000 Covid-19 cases by the middle of February. Where we go the remainder of this week will likely be telling. I refer the reader to the full portfolio of KHPI’s data visualizations on Tableau Public.
Testing and Test Positivity Rate (TPR).
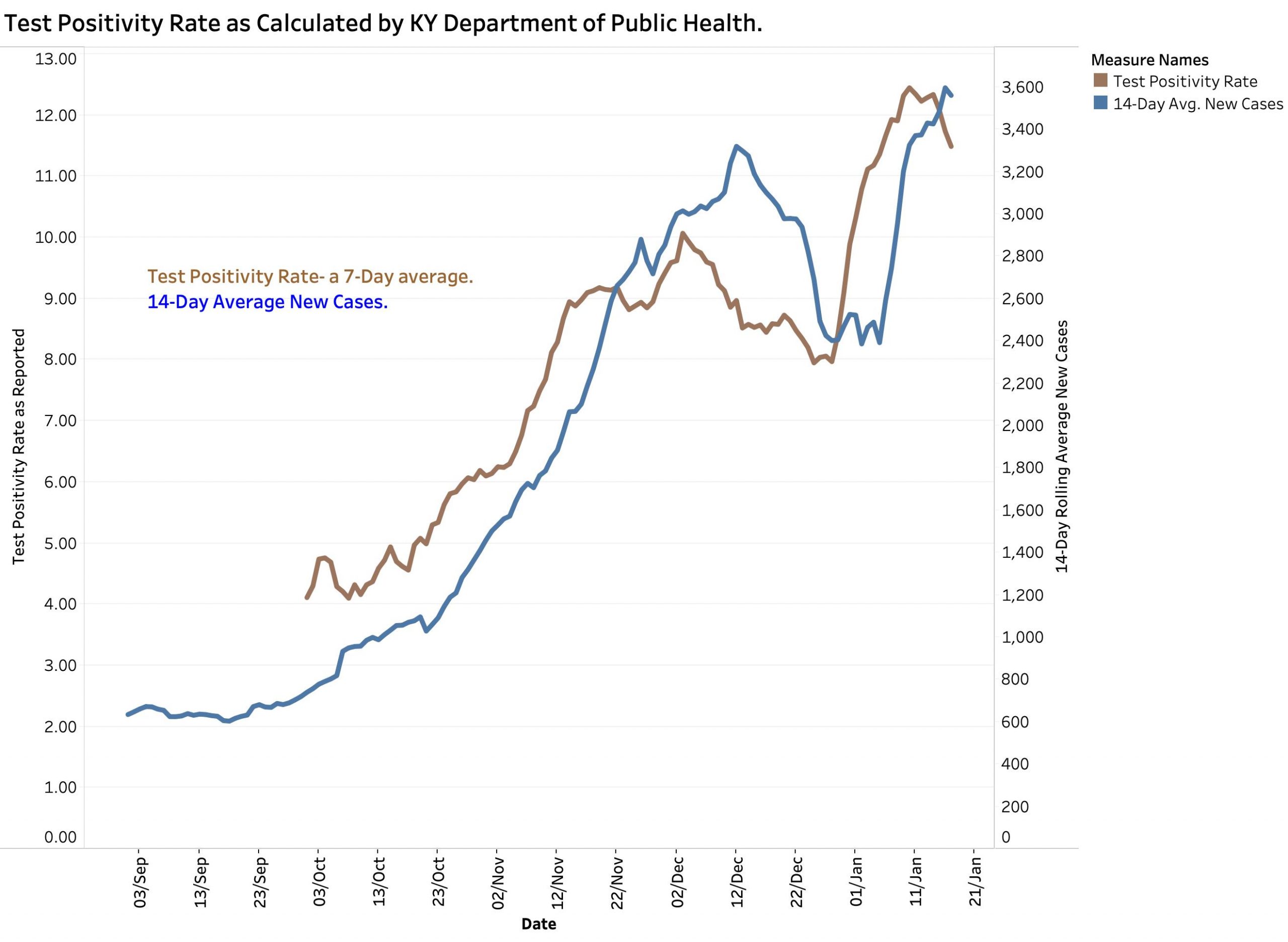
I manually entered the Test Positivity Rates reported by the state since early October into the KHPI database. To make daily calculation of this metric less volitile, the state includes only PCR Viral-RNA tests from swabs, and only from those testing centers that report to the state electronically. Although the major stated reason for calculating this measurement is to determine if enough testing is being done, it is also a truism that if the same kinds of people are being tested and the same number of tests are being performed, that the positivity rate will also reflect the prevalence of active Covid-19 disease in the tested population. Indeed, inspection of the graphic plots shows that the rise and fall of the 14-Day average of new cases tracks the Test Positivity Rate. At least since early October, new cases increased about a week after the Positivity Rate did, and correspondingly decreased when the Positivity Rate did.
The total numbers of weekly tests of all kinds reported has been relatively level the past month. We must keep in mind that the numerator and denominator of the TPR arithmetic are both averages and that what the TPR reflects will always be somewhat out of date. Additionally, I was able to confirm that there was a breakdown of the reporting system used by the state to receive electronic reports from its testing vendors. It is my understanding that workarounds have been in use for a duration undisclosed to me, and I must assume are still being used. I do not know the extent to which this computer system shortcoming effects other state and federal reporting of Covid-19 statistics. In my view, it is still the enumeration of new cases, deaths, and hospital utilization where the rubber meets the road.
Deaths.
Deaths that are thought to be due to Covid-19 are being reported at continuing high rates. Deaths lag the onset of individual infections by as much as two or three weeks. We may still be seeing the grim harvest of infections acquired over the Christmas and New Year Holidays– now three to four weeks behind us. Surges of cases may well still be occurring into 2021. The last full week ending January 16th set a record with 217 deaths. (Recall that there are additional deaths from unrecognized cases of Covid-19 and secondary “hidden” cases related to our healthcare system being turned upside-down.) At the rate we are going in January so far, we will end the month with 820 January deaths. The total number of deaths continues to rise exponentially, and if nothing else changes, by mid-February will have reached 4000 total deaths since the beginning of the epidemic.
Hospital Utilization.
Hospital, ICU, and Ventilator utilization had been sort-of level the last month, but if you have seen one hospital, you have seen one hospital! Each of our healthcare facilities, large and small, urban or rural face a unique set of challenges. They are doing the very best they can under worsening financial and staffing conditions and now with the additional responsibility to process immunizations.
The Cabinet for Medicare and Medicaid Services (CMS) is the interface between the federal government and hospitals. It recently issued an updated requirement for the individual hospital data to be reported to both state and the federal governments. I was frankly stunned by the number and complexity of the information required. From the perspective of a clinical investigator, this reporting required is the equivalent of a massive research project for which considerable time, personnel, and money is necessary to gather and report reliable numbers. I had this thought in my mind when I saw the anomalous spike in current ICU utilization in Kentucky from 403 to 548 in a single day with a drop to 392 the following day. The more complex the reporting scheme, the greater the opportunity for similarly questionable numbers to arise.
Endgame.
How bad does it have to get before we accept that we are not helpless in facing the current plague? There have been no breakthrough treatments for people with symptomatic Covid-19 disease although meaningful small advances are being made. We are learning more daily about the non-fatal and long-term nature of this disease. Surviving the acute phase does not necessary imply that a long and otherwise happy life will follow. What we do know is how to decrease the rate of new infections using public health practices that have saved our bacon for generations. Yes, they are not without cost to our psyches or pocketbooks. We will not know how bad this pandemic will be until it is over or at least controlled. Evidence from around the world and in our own country signals really bad. Which is the better choice? Letting the virus roll over us and wait to see what happens, or to try to minimize what is obviously happening to us. It is painful me to contemplate the enthusiastic willingness of Kentucky’s Republican-controlled legislature and Attorney General’s office to choose the former.
One very bright note.
The vaccines are here. The New England Journal of Medicine recently published the results of Pfizer’s initial testing of its vaccine which is now available in Kentucky! This is the data that allowed the FDA to release Pfizer’s vaccine to use by the public under an Emergency Use Authorization. I am much reassured by the results. There is no doubt of its effectiveness in preventing symptomatic infection and in virtually eliminating severe complications in people who got the vaccine when compared to those who got a shot of salt water. A few people who got the vaccine developed symptomatic Covid-19 but most of these occurred in the first 7-10 days after the first shot when it would be too soon to develop meaningful immunity. While even the first shot gave some protection, the second booster shot three weeks later sealed the deal allowing the claim that the vaccine was 95% effective. As for short-term side effects, these were acceptably minor, and to my surprise were not as bad in older people compared to younger ones. The vaccine appeared to be equivalently effective and safe in subgroups such as age from 16 and up, race and ethnicity, sex, body-mass index of obesity, or coexisting condition such as hypertension. I do not have permission to reproduce the article, but it is free on the journal’s website. I refer you to Figure-3 at the end. You do not need to be a statistician to see the dramatic effect on prevention of symptomatic Covid-19. [The blue line shows the increasing numbers of people who got the placebo shot. The red line representing those who got the vaccine becomes essentially level even before the 3-week booster.] The vaccine proved to be so effective that it was no longer ethical to not offer the vaccine to the volunteers who received the placebo. For my part, I want this vaccine or its equivalent!
Pfizer and the FDA will continue to follow the people in the study to investigate how long the protection lasts, and to make sure there are no significant long-term safety considerations. Importantly, there are plans or studies underway to determine if the vaccine also prevents asymptomatic Coronavirus infections, the shedding of viable virus particles that could infect other people, or its effectiveness in younger individuals. Until such information is in hand, it is reasonable to ask immunized people to continue to follow general public health measures. The more that people cooperate with such studies and public health measures, the sooner things will get simpler. Sadly, the availability of the vaccine to the general public of our nation has been sub-optimal for a variety of reasons– some unpardonable. We need to do some things differently.
Peter Hasselbacher, MD
Emeritus Professor of Medicine, UofL
Board Certification, Diagnostic Laboratory Immunology
18 January 2021
New cases appear to have turned a corner downwards. Deaths set new daily high Thursday at 58 and are projected to continue to for this week and for January but represent the impact of peak cases two to three weeks earlier. Will breath easier if case numbers move in same direction for the better after Saturday’s report to come. We could use the good news!
Peter Hasselbacher, MD
January 22, 2021