Prelude
I don’t remember three days of my life.
I have generally felt in control of my life and behavior. Although I understand the future is always uncertain, I do as much as I can to plan for it and minimize risk to myself and my family. This includes focusing on avoidance of stress, healthy eating, and daily exercise. Despite this, anything is subject to change at any time for no apparent reason.
On Friday, Oct. 25, following the Partners Connected Health Symposium in Boston, the Society for Participatory Medicine (an organization I co-founded and for which I currently serve as as co-chair of the board) hosted a reception for its members. This was followed by a dinner to kick off a retreat of SPM board members and a few guests to strategize around the future of the organization. Several of us spent months planning this event and we were anxiously anticipating it. Because we were ending the evening late and starting early Saturday morning, I decided to stay in Boston at the meeting hotel.
Saturday morning I awoke at 3am with severe vertigo (dizziness accompanied by the sensation that the room was spinning), as well as partial loss of hearing and low-pitched tinnitus in my left ear. I vomited due to the vertigo. At the time, I attributed this to having too much wine at the evening events, although I did not recall drinking much and these symptoms were highly atypical for me under any circumstances (I’m actually one of those people with a proverbial “cast iron stomach”). I was able to go back to sleep but awoke just before my alarm with the same constellation of symptoms.
I made it to the meeting by our 7:30am start, and apologized for what I felt was a hangover. The meeting went superbly, thanks to a great deal of planning by a fantastic team, an excellent facilitator, the participants’ engagement, and terrific food.
We adjourned around 4:30pm. I drove off and did my usual weekend errands, including shopping at Trader Joe’s and buying live crickets at the pet store for my daughters’ pets: Aussie, an Australian green tree frog, and Leonardo, a leopard gecko. (Even though the girls are off at college, it somehow still falls on me to take care of these critters.) I told Libby I wasn’t feeling well and only had a bit of dinner before we settled down to watch the Red Sox take on the Cardinals in game 3 of the World Series. The Sox were not playing their best (we eventually lost), I was tired, and by 10pm I went up to bed.
That was the last thing I remember.
I later learned that Libby heard what sounded like a fall, followed immediately by my footsteps, so she assumed all was well. When she came up to bed around midnight after we lost the game, I was sleeping peacefully in bed. I reflexly put my arm around her and woke up a bit. She took that opportunity to mention the bang she had heard, and asked if I had fallen or dropped something, to which I responded, “No, I didn’t fall; I didn’t drop anything.”
The Event
Ninety minutes later she felt the rhythmic pounding of my fists against her back. She turned to see a terrifying sight: My eyes were open but I was unconscious, my entire body was rhythmically convulsing, I was gnashing my teeth, and I had been incontinent of urine. While this would have been frightening for anyone to see, as a physician I have witnessed many generalized tonic-clonic seizures (formerly known as grand mal seizures). As a non-medical person, nothing could have prepared Libby for this. She feared she was losing me.
She frantically called 9-1-1, having trouble pressing the right buttons in her panic. For reasons I don’t understand she remembers being asked my age and little else. Then she was told to sweep my mouth with her finger (which I could have bitten off), drag me to the floor, and perform chest compressions. Thank goodness she is not stronger or she could have broken my ribs.
(I have since communicated with the local emergency medical dispatch supervisor. She reviewed the recording of the call. Based on the information they could glean from my poor panicked wife, which included that I was making gurgling sounds and was unconscious, the dispatcher made the assumption that I was having a cardiac arrest, which meant that checking my airway and doing chest compressions were, in fact, indicated. The situation reminded me of Law #3 from Samuel Shem’s novel House of God, which is “At a cardiac arrest, the first procedure is to take your own pulse.”)
Fortunately the paramedics arrived rapidly and assessed the situation. They assessed the ABCs, medicated my seizure, and transported me to Beth Israel Deaconess Medical Center, where I have been on medical staff since 1991. Living in a medical Mecca like the Boston area is a real blessing when you have a serious medical condition.
(Libby later told me that—even though she felt there was no evidence of my consciousness—she permitted herself a private happy moment when I escaped from the restraints the paramedics placed on me. I spent half my life performing magic and escaping from ropes, straitjackets, and other restraints, so she felt there was a part of me still present.)
There the staff soon whisked me off to have a head and neck CT with angiography (because of concern for acute stroke, cerebral aneurysm, or other acute cerebral pathology), and on my way back to the ER I had another seizure which required a great deal of medication to control. At that point I was intubated to protect my airway, which was fortunate because I then had a third seizure and required even more sedation and anticonvulsants. I was taken to the Surgical ICU, since we don’t have a dedicated neurologic ICU. This was very early Sunday morning October 27.
The preliminary reading of the CT angiography was:
“There is a hypodense region in the right inferior frontal lobe suggestive of an infarction with multiple small hyperdense foci
suggestive of punctate hemorrhages. The major intracranial vasculature is normal with no evidence of an occlusion, aneurysm, or dissection. There is however slight heterogeneity of the venous vasculature in the right inferior frontal lobe which is nonspecific but may be seen in the setting of a small developmental venous anomaly. This area will be further evaluated with reconstructed images. No herniation. MRI with GRE imaging may be obtained to evaluate for punctate hemorrhages elsewhere in the brain. Full report to follow.”
The final conclusion, which was released that evening following 3D reconstructions and careful scrutiny, was:
“No evidence for aneurysm or arterial venous malformation.
Right inferior frontal lobe hypodensity with punctate intraparenchymal hemorrhages and a small amount of subdural hematoma. This may be related to
subacute infarct or trauma.”
By that time, I had also had an MRI to further clarify the situation. When I later viewed the MRI, I was stunned to see what I call the “money shot.” This is an image (or images) that contain the key findings, usually marked up by the radiologists. Here was mine (note green arrows at top left, which on CT and MRI imaging represents the right frontal area, which may be better seen if you click on the image to view a larger version):
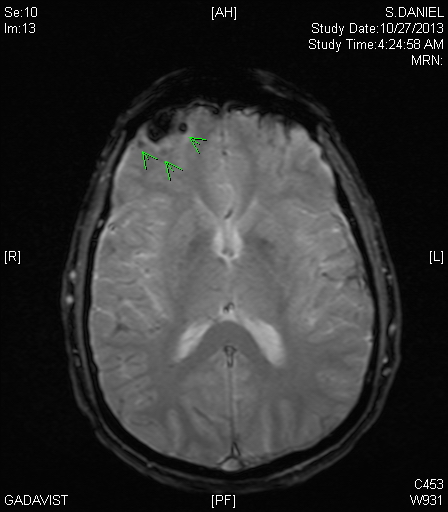
The interpretation was:
“Abnormality in the right frontal lobe with mild gliosis and enhancement and small amount of blood products. Findings could represent subacute infarction or contusion. Possibility of neoplasm is felt to be less likely but cannot be entirely excluded. Recommend followup imaging in four weeks to assess the temporal evolution of this lesion.”
Viewing this after my hospitalization, I was in denial that this could be me. How could this terrible looking image be my brain? Cancer? Stroke? I’ve seen many brain images, including many that were much worse than this. But these were of patients, not me. This can’t be me!
But at the time I wasn’t thinking anything; I was still unconscious and intubated in the ICU.
While there I had thousands of dollars worth of tests, including an EEG, an echocardiogram (with bubbles to check for shunting), a lumbar puncture with numerous tests for pathogens, various blood tests, and a follow-up head CT. But I was not aware of any of this.
In the meantime, I was extubated after about 12 hours since I was no longer seizing and seemed to be stable. However, although I breathed on my own and even spoke with people, I did not form new memories for almost two more days, as if I had a dementia. This could have been from the cerebral lesion, whatever it was, or it could have been from all the benzodiazepines I received to suppress my seizures. For example, my parents arrived from Florida just after I had been extubated, and I was just as surprised to see them on Monday morning as I was on Sunday night.
The good news is, I looked great :-/. Note the EEG leads all over my head. Thanks Dad for the flattering photography…

Going Home
Fortunately, by late Tuesday I was forming new memories again, and asked to be discharged because I didn’t feel like I would benefit from additional days in the hospital. My remaining deficits seemed to be some positional vertigo and some gait instability when I turned my head. I later realized that I also continued to have low-pitched tinnitus in my left ear and anything I listened to had an irritating quality to it. I also had a terrible headache.
I was told that I should remain on anticonvulsants for the time being and that Massachusetts state law forbade driving for six months following my seizure. I was glad that pharmacology had advanced quite a bit in the last twenty years—the previous choices of medications had terrible side effects and drug interactions, but newer medications were much easier to tolerate. Although not driving seems like a terrible inconvenience, I live near the Green Line, usually have meetings in Boston or within walking distance of my home, or take a taxi to the airport for my frequent travels. Most of my driving is to run errands on the weekends.
Because of the uncertainty of the diagnosis, I was prescribed atorvastatin to lower my LDL cholesterol and risk of future strokes. When I asked if they measured it in the hospital, I was told it was 107 (which is rather low already) so I politely declined. Besides, the imaging showed no evidence of plaque in my carotid arteries, my blood pressure was low, and I had no family history of cerebrovascular disease or coronary artery disease. I was also told to take a baby aspirin, which I reluctantly accepted, because it was a fairly benign intervention that has been shown to reduce the risk of coronary artery disease in men over the age of 50 (although we now generally only recommend it to those with risk factors). Once I was conscious and mentating it became much easier to be an e-patient.
And then came the bad news—at least for my lifestyle, which was top of mind for me because I had not yet grasped the clinical gravity and uncertainty of the situation. I was not permitted to do strenuous activity, for fear of increasing intracranial pressure, and I was not permitted to fly for the time being, because of possible risk for bleeding. I was advised to take some time off of patient care activities. I also was not to use alcohol or to take non-steroidal anti-inflammatory drugs. I would require follow-up evaluations to help determine my diagnosis. Finally, I was told I would need more sleep as my brain healed.
Libby brought me home and I contemplated my future.
Coping
I had already decided to go through with running a long-scheduled ninety-minute teleconference the following day that included about a dozen people. This was a task force I was leading on the future of AMIA, my professional organization. Although the EVP helping with this task force offered to postpone the meeting, I did not want to risk missing our deadlines. Besides, it would give me something to do. Fortunately, the meeting went very well.
But soon after arriving home, I reflected on what had happened to me and what the future may hold.
First it was difficult for me to grasp that I had had three seizures. A generalized tonic-clonic seizure is the ultimate loss of control. I witnessed many seizures during my residency, and always hoped never to experience one. A stray neuron in the brain triggers a cascade of neurons firing rhythmically, causing a loss of consciousness and all the voluntary muscles in the body to involuntarily and rhythmically contract. When it ends, the person is left in a postictal state in which there is an altered level of consciousness. In my case, because of the medications I was given, I never really regained consciousness at all. Talk about a loss of control! Even at my worst, I have never come close to losing control this completely. Reflecting on this has helped me empathize more closely with the dozens of patients I have cared for over the years who suffered from epilepsy.
Next, it was terrifying not to have a definitive diagnosis or prognosis, because the possibilities, based on the test results, were mostly quite frightening.
Finally, why had my body betrayed me? Didn’t I do everything to maintain my health? How could this happen?
Questions swirled through my mind, some prompted by having taken care of so many ill patients over the last quarter century. Although I felt fortunate that I had little in the way of residual neurologic deficits, would I worsen over time? Would I be able to continue to earn a living? Pay my kids’ college tuitions? Pay my mortgage? Travel? What if my seizures were uncontrollable—how could I ever take the chance of giving another keynote presentation? And if I wasn’t permitted to exercise, would I alter my metabolism and increase my risk for developing heart disease and other conditions? The brain is the source of feeling, volitional muscle activity, speech, comprehension, memory, personality, and thought. Although I could apparently control my muscles and had no sensory deficits, would my personality or memory be affected?
And then a logistical question: how and when should I tell people what happened to me?
I first made sure my practice knew that I would need to take some time off until I was cleared.
Since I spend most of my time as a consultant, I was very concerned about my long-term clients. I sent each of them an e-mail explaining what had happened to me. I did this despite my concerns about appearing vulnerable, because I felt that I owed them openness and transparency and trusted that they would be supportive. They were, and I am grateful for that.
But as I thought of my clients, my mind again took me to terrible places. One of them, Best Doctors, provides a second opinion service. Would I need this service to help determine my diagnosis and treatment plan? Another client, Kinergy Health, provides a platform and service to help informal and professional caregivers to collaborate and share information around the care of a person, often someone with serious chronic conditions. Would Libby need to use this to collaborate with home care agencies and my daughters as my condition worsened? And another client, SeniorLink/Caregiver Homes, trains and supports family caregivers so they can manage the care of patients that would otherwise be in a nursing home. Would Libby need this service to learn how to care for me as I became increasingly disabled?
Throughout my adult life I had always been an upbeat and optimistic person, but now I cried frequently as I contemplated the uncertain future. Was my brain injury causing me to be depressed or the situation itself?
Managing my symptoms was challenging. I had severe headaches and Tylenol did not help one bit. I was then prescribed Vicodin, which relieved the headaches but also made me feel loopy, sedated, and constipated. It’s hard to believe that this is a drug of abuse. I took as little as I could get away with, preferring relaxation exercises and a cool cloth on my head.
Every day, Libby (who was able to take some time off work to look after me) took long walks with me around a nearby lake. The fresh air, exercise, and change of scenery did me some good. And the more I spent time with Libby made me realize how special she was and what a terrible thing I put her through (although she reminded me that it was not my fault). I felt fortunate to have found such a wonderful soul mate.
Libby suggested we look for my disability insurance policy. The mere thought of it made me shudder.
As I thought about my condition, I realized that as much as I had done to take care of myself there is a great deal beyond one’s control. I felt vulnerable.
And we still didn’t know what had caused this or what was to come. My biggest concerns were malignancy, stroke, and vascular malformation, with a parallel concern being the potential for future seizures.
The Diagnostician
About a week after I left the SICU I had an appointment with the head of our stroke unit, Dr. Louis Caplan, an experienced and wise man who has been chief of numerous departments of neurology in his career and has a reputation as a brilliant diagnostician. Prior to the appointment I spoke with Dr. Jack Conomy, a neurologist and long-time mentor who initially inspired me to pursue a career in medicine, who called to wish me well. As luck would have it, he has known Dr. Caplan for decades.
Libby and I entered Dr. Caplan’s office, where we were introduced to four observers, each at a different stage of training, who were there to learn from the master. While not an uncommon sight in the hospital, having this many people in a small outpatient examination room can be a challenge.
Dr. Caplan asked dozens of questions of us, writing copious handwritten notes and creating a timeline. He then examined me and looked at some of the test results through the EHR. Then he rose and proclaimed, like Jack Klugman in the late 1970s television show Quincy, M.E., “There is only one thing this can be. Here’s what happened…”
He explained that my vertigo and tinnitus the night before my seizure was caused by a vestibular neuronitis, an inflammation of the eight cranial nerve (in retrospect, this made much more sense than a hangover). When Libby heard a fall, I had in fact struck my head. But the fall caused a retrograde amnesia so I did not remember it. The impact caused a contusion in my right frontal lobe (but no external signs of trauma). As the contusion grew in my head (much as a bruise of an arm or leg gets more swollen over several hours) it disrupted the nerves enough to trigger seizures. He felt the prognosis was excellent, did not think I was at risk for further seizures, and felt that I could exercise, fly, take NSAIDs, and see patients. He was so confident that he didn’t even think I needed the follow-up MRI that was already scheduled, but he understood if we still wanted to have it for peace of mind. He wanted to see me again a month or so later.
I subsequently saw an epilepsy specialist who concurred that I was not likely to have ongoing seizures, but still recommended six months of anticonvulsants before weaning, just to be safe. And I still was barred from driving, by state law.
Recovery
Having been told that my prognosis was good immediately lifted my spirits. I resumed exercise (although I’m still working on regaining flexibility, strength, and endurance), ramped up my work, reconnected with clients, managed patient messages, and prepared for upcoming presentations.
I had been planning to attend an upcoming conference, the AMIA Annual Symposium in Washington, DC, at which I was to speak four times. But I still had work to do. I changed my flight to a train ride and hoped that I would be able to make it, but was apprehensive. I knew this would be my first time away from Libby, who had been at my side constantly since my illness. And while there I’d be constantly “on,” interacting with people and attending events. Even worse, I had fallen behind in my schedule to complete my presentations.
But with a clearer head and assurance that my prognosis was good, I was better able to concentrate and focus on my work and my wellness. Every day my headaches and vertigo seemed to improve, and the tinnitus, while still annoying, became easier to tolerate. I still firmly believe that attitude matters, and I refused to give in to this thing, whatever it turned out to be.
Fortunately I finished my preparations and on Friday I anxiously took the long train ride to DC.
Returning to Danny
Attending the AMIA conference was a major test for me. How would I manage the travel? The constant interactions with colleagues? Public speaking? Fortunately the trip went well.
Traveling was not a problem, nor was taking public transportation or walking to my hotel. I had dinner with my daughter the night of my arrival. Seeing her after this ordeal was rejuvenating.
Saturday afternoon I helped teach a tutorial on consumer health with two dear friends, one of whom knew about my hospitalization and the other I told a few minutes before we co-presented. The tutorial was well received, and the most reassuring thing I heard after our tutorial was when one of my colleagues said that my presentation skills were back to at least 100 percent of my prior capacity. That certainly bolstered my confidence.
That night, I shared a taxi to a leadership dinner with e-Patient Dave, whom I would be introducing the following day for his keynote presentation. He already knew what I had been through and had been quite supportive. Although we already had a close working relationship (in both the clinical and professional settings) this was the first time that we were able to relate patient-to-patient.
Sunday morning was another breakthrough. I have been a runner for many years. But following a soccer injury to my left foot in June I had to immobilize my left foot and had not been permitted to run. Just as I was about to be ready to try running again, this illness arose. Since I was initially told not to exert myself, I did not know if I’d ever run again. For the first time in almost five months I ran: north on Connecticut Avenue and through the National Zoo. It felt fantastic.
At the opening plenary session that afternoon, I introduced Dave. I started with the slides I had designed two months prior, drawing a parallel between John F. Kennedy’s famous speech delivered at the Berlin wall, in which he expressed solidarity with the people of Berlin by stating “Ich bin ein Berliner,” and e-Patient Dave who proudly states “I am a patient.”

I then told the audience how true these words are: that only three weeks prior to this presentation, I was intubated in an ICU.
I spent a great deal of time at the conference embracing and greeting friends and colleagues, some of whom I have known for decades. This was extremely emotional for me, since until that time I wasn’t certain I would ever be able to see them again. I looked each one in the eyes and actually saw them like never before. Although I reliably met them at this conference year after year, it took an event like this to shake me up and realize that we must never take our friends for granted.
My other presentations also went well. Without a doubt, this was the most personally meaningful AMIA symposium I have ever attended.
A few days after returning to Boston I was scheduled to resume seeing my primary care patients. On arrival in our practice, I was immediately struck by the chaos, the barrage of paperwork (yes, paperwork, as anomalous as it seems in a relatively high-tech health care facility), and the stress, and even began to ask myself whether I should consider abandoning my clinical practice. But once I started seeing patients again, connecting with them, and helping them with their medical problems, I remembered why I had become a physician in the first place and why I must keep practicing.
Epilogue
I continue to improve daily. I focus on wellness and work and do not dwell on my lingering symptoms, something that I counsel all my patients to do. Attitude and lifestyle choices aren’t everything, but they matter a great deal. As the existentialist Jean-Paul Sartre said,
“What is important is not what happens to us, but how we respond to what happens to us.”
It is likely that someday each of you may encounter worse trials than mine, although I hope that you don’t. These are the times when the backbones and hearts of our family members are tested. We cannot know the challenges they will be given; we can only teach them, love them, and hope they do well through all life brings.
While I admit that my initial depression improved by being told that my prognosis was more favorable than I had expected, either way I would have coped in the only way I know how—through positive attitude. For even when reality is challenging, we must find a way to manage.
Many life lessons I learned from running. At times in a race I am confronted with what appears to be an insurmountably large hill, sometimes when I am already fatigued. If I keep looking at that big hill in front of me it will most certainly get the better of me. But if I keep my head down and focus on the ten feet in front of me, before long I will be at the summit. Many of life’s challenges can be approached that way, once you eliminate negative emotions.
Indeed, it is possible that the brilliant diagnostician I saw was incorrect (we’ll know when I have a follow-up MRI next month), but mentally it is better for me to focus on healthier thoughts and to ignore the possibility of bad news. Negative thoughts are toxic, both physically and mentally.
One friend I saw recently asked if this was a life-changing event for me. It certainly has been.
First, I think about it constantly, and contemplate my family, my friends, my career. I am fortunate that I have no memory of any of these terrible events, but am sad that my wife and family will never be able to forget them.
Next, although I have always been one to live life to its fullest—I adhere to Mahatma Gandhi’s dictum,
“Live as if you were to die tomorrow. Learn as if you were to live forever.”
This experience made me appreciate each day all the more.
Finally, this event has certainly helped me empathize with my patients even more, especially those with uncertain but potentially fatal diagnoses and those with seizure disorders. While every health care provider should, at some time in his or her life be a patient (recall the 1991 William Hurt movie The Doctor), I think being intubated in an ICU is going a bit farther than I had in mind.
As many have written, it’s difficult for physicians to be patients, because we tend to think of ourselves as immune to the maladies of our patients. But experiencing the patient’s perspective is truly valuable on many levels. For me the biggest lessons were experiencing the loss of control, an uncertain future, and vulnerability.
Even if I only can remember the experience following the three days that I can’t remember.
Read the follow-up here

Holy mackerel. Best wishes to you. I would never wish being a patient on any M.D., but oh, it gives us such a better perspective on our system and on life in their shoes. And how fascinating that your brilliant diagnostician spent the most time with that holy of all holies – the medical history. Rare these days……
(ps I am a friend of Dave’s and thus have been aware of your relationship)
Thanks, Bev. I agree with you–we should spend more time listening to our patients and asking questions and less time reflexively ordering drugs and tests.
> either way I would have coped in the only way I know how—
> through positive attitude. For even when reality is challenging,
> we must find a way to manage.
Fittingly, in a comment today on Susannah Fox’s latest post, I learned of a post written this month by SPM member Catherine Rose PhD, mother of a multiple-complex-condition child with severe challenges: Te Toca A Ti – It’s Your Turn. Powerful advice on dealing with what life hands you.
Thanks, Dave. Will check it out.
Have a healthy recovery Dr. Sands and God Blessings.
Muhammad Nauman
Thank you, Muhammad.
Dear Dr. Sands,
Thank you for sharing such a personal story. Your transparency is so very valuable and indeed it’s a powerful example of how we all can become patents so very quickly. Thank you for your work.
All My best,
Lisa
Escaping from the restraints! – Awesome!
Yes, it’s probably the only time Libby smiled in those three days.
Powerful Danny. So glad you’re still with us…
Thanks, Gregg. Me, too.
Dr Sands, Ironically I talk about being inspired by ePatient Dave, but likewise I learned from your interactions from ePatient Dave that great doctors are out there! Thank you so much for sharing your story, so so so very much. So glad you made it through safely and are back regaining steam. We are all fragile – but few are brave enough to boldly share it.
Thanks for your comments, Catherine.
Danny, I am so relieved to hear all upward tends continue! Everyone who cares about you has been waiting with bated breath, while trusting your innate resilience would also make quite a difference. Especially loved what you said about avoiding downward spirals of negativity; it is such a pit filled with quicksand, no? Be well and keep on bouncing!
Yes, positivity is really important in all of life. Thanks, Carla.
So glad to hear that the news is good and I hope it continues. Thanks so much for sharing your story. I had a family member with severe epilepsy, and it is truly a difficult one on all levels. Glad to know you will still see patients as you seem to be a rare provider from what I have seen and the world needs more like you. Best wishes on your continued recovery
Thanks for your comments and well wishes and I am sorry for your suffering family member. Very difficult condition.
As one of your Jr. High and Sr. High classmates, I want to wish you a full, speedy recovery. As someone with chronic illness I know how important a positive attitude is toward coping with long term symptoms. It also helps those who support us put up with us. lol 😉 I wish you and your family Abundant Blessings, Happy Thanksgiving, & Happy Hanukkah!
Nice to hear from you, Teri. It’s been awhile.
Sorry about your chronic illness. Please check out the Society for Participatory Medicine–we’re trying to make healthcare better.
Harrowing story, beautifully told. Thank you for sharing it, Danny!
Thanks, Susannah. It was great getting together in DC.
Agree with the Holy Mackerel- in fact it’s a Holy Mackerel times two!…and I am so glad you were able to see such a fine clinician as Dr. Caplan – it sounds like he really knows how to listen to a patient and reconstruct events taking all the info into account (the loud bang of your head on the floor!). I am happy you are back to Danny and things are looking very positive indeed. Thanks for sharing this amazing story (and thanks to your dad for the pic). Pat
Thanks, Pat. Yes, we need to spend more time listening to our patients.
Interesting that you’re thanking my dad for the picture–Libby was not happy that he took it.
Danny,
I am so sorry to learn about your health issues. I wish you a speedy recovery.
All my best,
Alice
Thanks, Alice.
Whoa! i didn’t know what you went through, Danny. We had a pretty nonchalant hallway conversation at AMIA… you certainly didn’t sound like a guy who went through an ordeal. Hats off to you..
Wish you a speedy recovery.
~Pallav
Well I didn’t want to wear it on my sleeve (although I felt like I told so many about it at the meeting.
Thanks for your good wishes.
Holy shit, batman. That’s a hell of a secret shopper experience, shows your dedication to checking out BIDMC from all angles!
More seriously, amazed to hear about this. Very glad that you are doing fine and very glad that you wrote about this (and of course even gladder that you are able to). Have a great thanksgiving, Matthew
Thanks, Matthew. I really appreciate it.
I thank you for sharing your recent experience, Dr. Sands.
Your ability to be transparent is absolutely inspirational. And I believe everything in life happens for a reason. As long as one makes the best use of an experience by promoting the valuable lessons learned and helping others somehow, then our true purpose is served. It seems that you already recognize the same. I pray for your holistic healing and hope you continue to spread the goodness through your works. GOD bless!
BTW, some experiences are better-off when left forgotten & behind. So, it is best to continue moving forward and cherish loved ones.
Best,
Shefali
Thanks, Shefali. I agree that it’s important we learn from all our experiences.
Inspiring and I think you need to add a demonstration of escaping from restraints to your next AMIA presentation. My own experience as a patient was eye opening but my experience as a caregiver and spouse opened my eyes even wider.
Danny,
I hope this is one of your best of many Happy Thanksgivings going forward. Thank you for a very powerful, well written scary, hopeful story.
All the best to you,
Jack
Thank you, Jack. That’s the way we feel.
Wow, Danny! What a frightening experience. Glad to hear all has been sorted out and you’re on your way to a full recovery. Here’s to a very special and particularly meaningful Thanksgiving.
Hugo
Thanks for the good wishes, Hugo. Hug your loved ones.
I remember meeting you and Dave deBronkart in Copenhagen a few years ago at a Patient Safety Conference. You were both such a breath of fresh air.
Thank you for telling your story so honestly. There was much I could relate to, both as a caregiver for a patient (my deceased husband) and as a patient myself. I woke up one Monday morning in 2010 with no memory of the last 24 hours. A quick overnight stay at the hospital with all the trimmings gave me a clean bill of health, and a couple of talks with a therapist confirmed that it was most likely stress related, going all the way back to my husband’s death 4 years earlier. We idenfied a couple of triggers that I could work on to prevent recurring events. But it was a long, long time before I stopped fearing the future, especially as I live alone.
This is what we all fear the most: the loss of control over our own lives, and the loss of control we feel as caregivers for those who are important to us; when all we can do is watch and wait and hope for the best. I try to make it very clear how frightening this is when I’m out telling my husband’s story as a WHO PFPS Champion. It is far from obvious to many in the medical community.
But in a crisis we all need to act, to do something about it – the hardest job for anyone is to do nothing and just wait for the outcome. Fear grows in that vacuum, so ANYTHING we can do is helpful – it keeps our spirits up.
I shall remember Dave’s proud statement “I’m a patient” when I next I tell my husband’s story to a bunch of freshly educated doctors two weeks from now.
Thank you for sharing your story.
Brigit, I do remember meeting you in Copenhagen. Your observations are spot on.
Dear Dr. Sands,
Thank you so much for sharing your story, and the poignant insights that have resulted. Five years ago, I lost my memory for about three months due to a concussion– was able to walk around and do things, fortunately, but could not hold a thought in my head for more than minutes at a time. It is a difficult experience to know that there is a block of time from your life that you will never remember. I’ve become thankful for it over the years as it has made me more appreciative of the good memories that happen each day. Reading your story here, I am thankful that you are on the road to good health again, that your (already-strong) sense of empathy has been re-energized, and that you are here to continue to lead the charge for better care.
Happy Thanksgiving, and thanks again for sharing.
Best,
Carolyn
Thanks for your comment and I am glad you’re doing better.
Thank you for sharing this experience, Dr. Sands. I lost three months of memory to a concussion five years ago, and I understand the uncertainty and fear that can come with an episode like that. It is not an easy thing to face, and it is certainly not easy for the ones you love either. I am thankful for it in retrospect, because it made me all the more appreciative for the good memories that I create on a daily basis. Very glad that you are on the mend, and I’m thankful today for empathetic, caring, and honest physicians like you. Best wishes for continued healing.
@DrDannySands thanks for sharing…raw, emotional, and i think important coming from an MD who does the type of work you do in healthcare.
At @AMIAinformatics Nov 2014 conference we need to have the second annual “to-be-named” run-we’ll make it happen-what say you @DrDannySands?
Thanks for your comment, Jeff. I’m game for the run!
I admire the eloquence of your story and am thankful, on this day of thanksgiving, for what seems like a happy ending in all respects. I have always seen you as someone happy, healthy, and fulfilled, so it is a bit of a shock to read what happened. One of my obsessions these days, because of events in my family, is what to say to patients and caregivers when you want to express your caring and concern but don’t know what to say. I want to let you know how moved I am by what you and your family suffered and how grateful for your reflections here.
Thanks, Lisa. Good luck with your family health issues. And keep pushing the communication agenda!
As a patient and caregiver: Just say what comes to mind – don’t make a song and dance about it. Practice makes perfect. I can’t count the healthcare professionals who have clammed up or spouted cliches when talking to me, both when my husband was alive and when I go out to tell the story of how he died (partially from medication error). It becomes embarrassing for both parties.
Better say something clumsy than say nothing, or fall back on standard cliches which sound hollow. If you say it with honest feeling THAT will get across.
I have practiced this myself, and have learned to rush in where angels fear to tread. It is (practically) ALWAYS appreciated.
Yes, Birgit, it is hard for many people to speak from their heart, especially when they are uncomfortable with a bad outcome. As Mark Twain said, “When in doubt, tell the truth.”
Danny – Wow! Your story is beautifully, compassionately and articulately written. You are so very lucky in many ways. And you are so right about positivity (Barbara Fredrickson is a researcher with a book on this). When my cousin was diagnosed with melanoma he called me wth his two biggest fears – being in pain and losing control. We worked with his wife and physicians so he could live the next four years with options. Thank you for sharing this with us. Have a gratitude-filled Thanksgiving.
Thanks for sharing your story, Maggi! and for your kind remarks. Hope to see you soon.
Thanks Danny, you are an inspiration to us all. I did not notice you missing a beat at the AMIA meeting, and now I realize further why your work and now your life is an inspiration to us all in informatics and beyond. Happy Thanksgivvukah!
Thanks so much, Bill. Best wishes to you and your loved ones and to all you touch in your work.
Danny, thanks for sharing your story. Glad your recovering…we need your voice in the patient movement!
Thanks, Maureen. I look forward to future collaboration with IHI.
Beautifully written, Danny. Happy Thanksgiving, my friend. See you soon.
Thanks, John. See you soon.
Danny,
You inspire all of us, not only through this experience, but because of who you are. May you continue to go from strength to strength.
Thanks for the kind words, Nancy. See you soon.
Danny, having spent time with you – although not as a patient – you are indeed an uber optimist (from fellow optimist) but I also saw how vigilant you are about the well-being of those you care for, and care about. Your writing this is but another example: sharing the
unthinkable and what happened after. And now, on this (U.S) Thanksgiving Weekend, a question in the spirit of emails and twitter abounding with Engage with Grace and The Conversation Project and Death over Dinner: do you have an Advance Directive? Your experience gives me pause for thought in my own BestEndings journey.
From Canada, I am giving thanks that you’re feeling ever weller. Kathy
Yes, we must all plan for the unthinkable, ideally when we’re well. Thanks for the good thoughts, Kathy.
This is extraordinary. Thank you so much for giving us this amazing piece!
Enclosed please find our deepest best wishes that all continues on the upswing, for you — and for your family and loved ones, including and especially for our good friend friend epatientdave.
Thanks, Jeanne. I’m feeling the love.
Wow! Glad to hear you are doing well! You are missed here at the big “C”.
Thanks, Paul. Send my regards to the team there.
Dan- Nothing like a brush with mortality to remind us of the transient nature of human existence. We are so glad that you have persevered and are improving daily. I was personally hoping you would be even better than before(fewer card tricks) but that may be too much to ask. Tell Libby she can forego any planned stress tests this year. No need.
With all our thoughts and prayers and gratitude for your recovery.
The Cutlers
Thanks, Dave and Robyn. Good wishes and good humor–well done. I’ll try not to stress out Libby so much in the future (but it’s hard being married to me).
Whoa Danny!
It took me a while to believe you were actually talking about you. We will all be patients one day. So glad you have the opportunity to not be one now, what a great gift. Enjoy it, you deserve it, thanks for everything,
Ted
Hard for us to believe, as well–still! Thanks for your good wishes. We’re crossing fingers for a good MRI in a few weeks. Hoping to see you soon.
Danny, what a story! I’m sorry you and your family have had to go through this and so glad to hear that you are improving. I join others in thanking you for your clear and honest reporting and sending best wishes for follow-up testing. Love the image of the magician in you escaping the restraints!
Great to hear from you, Susan. Thanks for the comments.
Danny,
Good to hear your voice! Thanks for adding to the body of patient lit, and I’m very glad to know you have a good prognosis and – wait for it – GOOD QUALITY OF LIFE 🙂
One of the “hangovers” for me of being both patient and caregiver has been the “woulda-coulda-shouldas” nag of hindsight. Most problematic are the times we and our caregivers and providers observed symptoms and thought horses, not zebras. Did we delay care? Put the patient’s outcome at risk?
I’m not seeking a solution, just wondering aloud if others waste as much mental energy thinking about this as I fear I do. I appreciate that you’re focused on mindful living and staying optimistic.
Keep the faith!
I think your fears are normal, Eve, but usually these are horses. More importantly, you can’t spend your life looking over your shoulder–it will eat you up. So you do need to advocate for your loved ones and ask questions as they arise, but you can’t expect that you’ll be perfect.
Thank you for this touching story. I also had a seizure, although just one and I was awake shortly thereafter. But I can certainly relate to the feeling of complete loss of control and wondering what the heck is going on, but at the time and in the months that followed.
*both, not but 🙂
That was very scary and the outcome is still unknown, but a blessing nonetheless. I’m thankful you are my doctor. I thank your wife for her alertness her input was invaluable to the diagnosis.
Happy Holidays!
Wini
Thanks, Wini. Happy and Healthy Holidays to you and your loved ones.