
Sept 30th update and correction
The post below was written shortly after I learned of the events in Charikot. Turns out the patient was two-and-a-half years old, not a newborn. There have been other developments – all the doctors have left; the local political authorities did not seem to have taken the proper action; the video has been roundly condemned; the hospital is presently shutdown; and the family has expressed the idea that they did not want such a drastic outcome. The Ministry of Health has sent a three-person committee to Charikot.
It’s more than I can keep up with. I need to resist the urge to relay each new development breathlessly before the next step develops.
For me, the bottom line remains that the young doctors needed more preparation for their posting, then they got. For five years I have worked to promote the need to teach situational awareness. I am hoping that if there is any good to be gained from, it will be when the Ministry of Health, The Nepal Medical Association, and the medical colleges take a good look at how to introduce this into the curriculum for all MBBS doctors in Nepal.
Charikot Incident
In Charikot, Dolkaha district of Nepal, the hospital staff are under investigation due to an incident in which a newborn baby (correction: 2 1/2 year old) died after being brought to ER. It is not unusual to have a person die in an Emergency Room; in this case the family reacted by blaming the hospital staff and threatening them. This too, is not unusual. Any Nepali nurse can tell you this or that incident in which this was a problem.
In Charikot, none of the staff seem to have been hurt (we await more details) but the whole incident was traumatic. The local authorities are investigating.
I’ve been through Charikot, on a “local” bus. It was the last east-bound bus of the day. We were all headed to Manthali. http://wp.me/p1pDBL-pK The bus was overfull. Such buses always are. The bus crew did not want anybody on the roof. About a dozen guys wanted to ride the roof. There was an argument and a lot of shouting and jostling. The guys got on. Rural Nepal is not always Never Ending Peace and Love.
Back to the incident at hand
start with a recent video:
(update: evidently the acting district officer was unable to disperse a crowd of 300 people who had gathered, and ordered the doctors to do this, recording this video. This is unprecedented in Nepal). The hospital in Charikot was damaged in the second big earthquake of 2015, May 6th, when the epicenter was in Dolakha district. Since then, it has been a project of the US-based NGO, “Possible Health.”
Here is the website of Possible: http://possiblehealth.org/rebuilding-nepal/ They are doing good work in a critical sector. The NGO is “foreign” but the staff is Nepali. ( update: and most of the members of their Board are Nepali).
The link above includes a description of their work in Charikot and rebuilding health posts in that region. There is an informative Q & A.
Press Release
Since the incident, there is a press release from Possible Health:
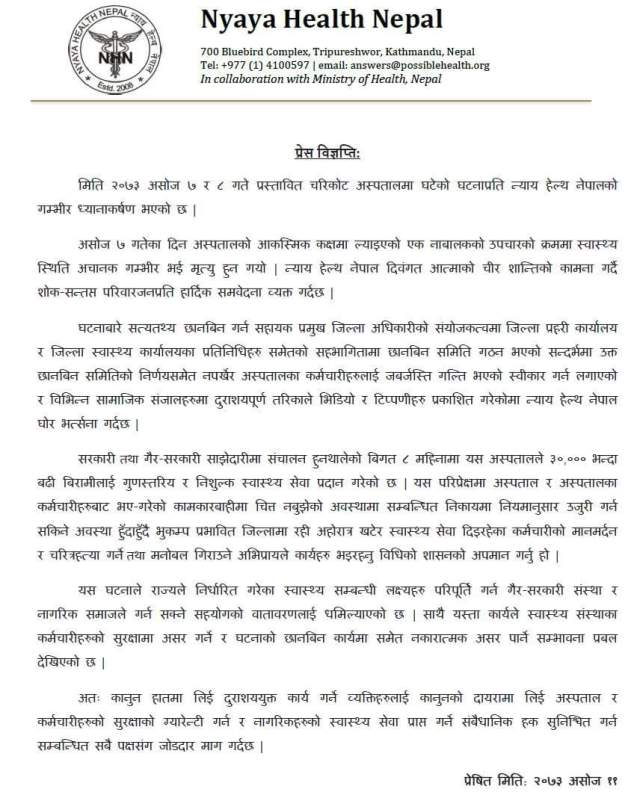
This describes the incident. In Nepali of course! I do not presently have an exact translation.
My friends from Possible were shocked.
For me, the story is familiar. A critically ill person is brought to the ER. The family demands the staff to do something, but it is too late and the victim dies. Somehow the family demands that the staff be held responsible. Things spiral out of control.
A lot of my work in Nepal is to prepare nurses and doctors for appropriate handling of this situation, and in fact, CCNEPal has trained 2,885 nurses and doctors as to how to respond when this exact thing happens. We do this by incorporating a scenario-based approach to the principles of counseling the patient party.
Critical fact!!!!!!!
This happens all over Nepal. It is not the first time. It is more highly publicized than most of the other times.
One important thing to know is – the doctor(s) will always be blamed regardless of the facts of the case. Anger is a predominant response in acute grief in Nepal. These incidents have a history of happening throughout the country and they are depressingly familiar.
My second book about Nepal, The Sacrament of the Goddess, depicts just such an event and it’s the climax of the book. https://www.amazon.com/Sacrament-Goddess-Joe-Niemczura/dp/1632100029/
Nepal is Hindu and Buddhist. This novel explores the issue of how people reconcile with anger and violence in a country known for peace and love.
Preparation is critical for an effective response
It takes courage to be an ER nurse or ER doctor in Nepal. You need more than just the ACLS protocols.
Some hospitals already train their staff. They are considerably less likely to have this problem. Or at least it will be mitigated.
First, take a look at this YouTube playlist:
https://www.youtube.com/playlist?list=PLSXynKNP9Lj_nhaj4P-KnR4nVYu6cub-7
Past blog entries with practical suggestions
next, on this very blog are a dozen or more entries on the subject of how to
prevent thrashing and to maintain an secure environment.

MBBS students participating in a role play. Here, they are security guards bringing an unresponsive “victim” for emergent care. Other participants play the role of distraught family.
If you only read one, it should be this:
http://wp.me/p1pDBL-v3
ten rules:
http://wp.me/p1pDBL-Ny
My response after the incident at Patan Hospital:
http://wp.me/p1pDBL-Cu
Hospitals during Nakibanda:
http://wp.me/p1pDBL-BV
Campaign to teach situational awareness:
http://wp.me/p1pDBL-Bb
I’ll try to follow the outcome of this incident. I hope it does not deter Possible from continuing the excellent work they are doing.
S
